

Pituitary Pars Intermedia Dysfunction (PPID)
Takeaways
- PPID is an age-related endocrine disorder common in older equids.
- PPID is caused by degeneration of neurons that affect the production of hormones such as adrenocorticotrophic hormone (ACTH).
- Common clinical signs include a long, curly hair coat, delayed shedding, loss of muscle, poor immune function, and laminitis.
- The only medication licensed for the treatment of PPID in horses is pergolide mesylate.
- There is no cure for PPID. Management through medication, diet, and exercise must be maintained for the life of the animal.
What is pituitary pars intermedia dysfunction?
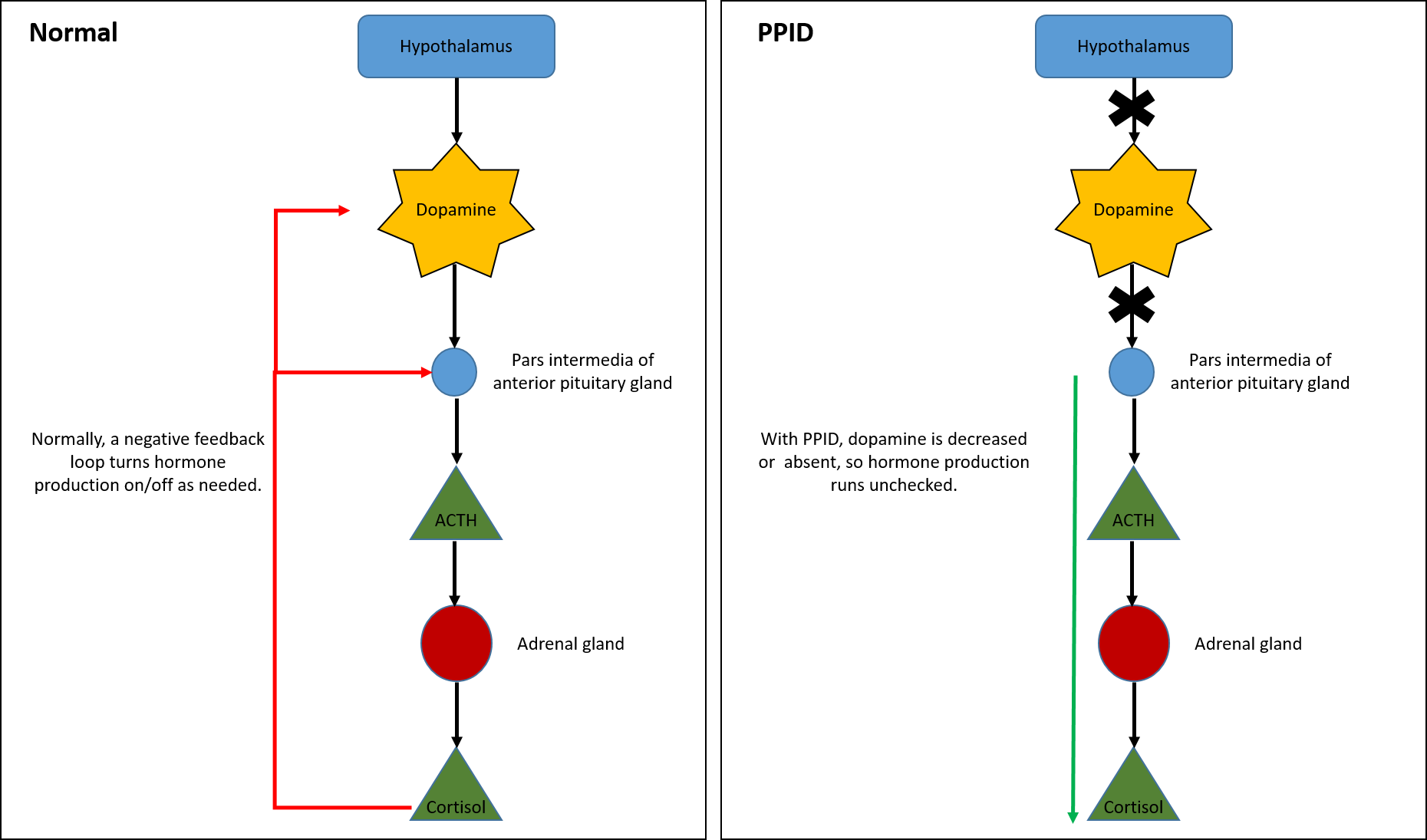
Pituitary pars intermedia dysfunction (PPID), also known as Cushing’s Disease, affects hormone production pathways in the brain, specifically from the hypothalamus and pituitary glands. The release of hormones from the pituitary gland is normally controlled by the hypothalamus through the neurotransmitter dopamine. With PPID, the degeneration of neurons that produce dopamine results in an inability to control the hormones produced by the middle lobe of the pituitary gland (pars intermedia). High levels of these hormones affect processes throughout the body.
The disease is age-related, with cases typically occurring in horses older than 15 years of age, although horses as young as 7 years of age have reportedly been diagnosed with PPID.
To date, aging is the only significant risk factor for PPID. There are no breed or sex predispositions.
What are the clinical signs of pituitary pars intermedia dysfunction?

The most common clinical signs of PPID are a long, curly hair coat (hypertrichosis), delayed shedding, loss of muscle (especially along the topline), abnormal thirst (polydipsia), excessive urination (polyuria), lethargy, and laminitis. Sometimes delayed shedding starts with longer hairs on the legs or under the throatlatch. Additional signs may include a rounded abdomen (potbelly), exercise intolerance and abnormal sweating. Affected horses may have fat deposits on the top of the neck, tailhead, and above the eyes. Horses with PPID can be susceptible to chronic infections (i.e. skin infections, pneumonia, sinus infections) and abscesses, have decreased wound healing, and have higher parasite burdens.
Approximately 30% of horses with PPID also show signs of insulin dysregulation. In these horses, blood insulin levels are high because tissues have a decreased insulin response. Insulin dysregulation is the hallmark of equine metabolic syndrome (EMS), and PPID and EMS can coexist at the same time in a single animal. Knowledge of insulin status is important for assessing laminitis risk and informing dietary management.
How is pituitary pars intermedia dysfunction diagnosed?
Diagnosis of PPID is based on the presence of clinical signs along with diagnostic testing. Although early intervention is paramount to avoiding negative consequences from the disease, detection of early PPID can be challenging since clinical signs may be vague. A variety of tests, or combination of tests, can be used for diagnosis:
Baseline ACTH test - A blood sample is taken to determine the level of ACTH in the plasma, which is compared to an established reference range. Horses do not need to be fasted, but should not have consumed grain within 12 hours prior to the test. An increase in ACTH concentration in the fall is normal, and testing during this time requires utilizing appropriate seasonal reference ranges. ACTH concentrations can vary with stress, illness, exercise, and sometimes diet, so testing the horse at their home environment when they are healthy and not stressed is ideal. A baseline ACTH test is good at detecting moderate to more advanced cases of PPID but may not pick up horses early on in the disease process.
Thyrotropin releasing hormone (TRH) stimulation test - A baseline ACTH sample is collected as described above, TRH is administered intravenously (IV) and another ACTH sample is collected 10 minutes later. This may be a good test for early PPID, or when ACTH testing is inconclusive, but there can be substantial variability.
Since PPID and EMS can coexist, it is also important to test for insulin dysregulation.
How is pituitary pars intermedia dysfunction treated?
It is important to note that there is no cure for PPID. Treatment is intended to reduce clinical signs of the disease and must be continued for the life of the animal.
The only medication licensed for the treatment of PPID in horses is pergolide mesylate. Compounded pergolide formulations have been shown to be highly variable and unstable over time. Prascend® is the only FDA-approved pergolide formulation for horses. Clinical signs should show improvement within 1-3 months. Horses that do not respond to high doses of pergolide may also require cyproheptadine (Periactin). Ongoing monitoring is important and retesting should be performed at least twice a year, with one assessment during the fall, to determine if there is a need for changes in medication.
Management of PPID-affected horses also involves a veterinarian-approved diet and exercise program. The horse’s body condition score (BCS), ability to perform exercise, and whether or not insulin dysregulation is exhibited all affect management approaches. As horses age, feed requirements and types of feed (i.e. hay versus pellets) may change over time and should be discussed with a veterinarian. Horses with PPID should also receive good preventative veterinary care to ensure they are healthy due to a decrease in their immune responses. This includes a regular deworming and vaccination protocol, routine dental examination, and periodic blood work if possible. Regular farrier work is also important, particularly if animals have had bouts of laminitis as a consequence of PPID.
Finally, horses with PPID that is harder to control also benefit from body clipping and access to shade with good ventilation in the summer since they may sweat more due to a long coat. It is a common misconception that hypertrichosis (excessive hair growth) in horses with PPID (which makes it harder to lose heat in the hot months) means that PPID horses run hotter. In rare cases, PPID horses lack the ability to sweat, and so are more susceptible to heat. In even rarer instances where there may be degeneration of the hypothalmic temperature control center, this will result in a true inability to regulate temperature (up or down). There is currently no concrete evidence of this in PPID horses and it is independently exceedingly rare. For the winter, PPID horses should be treated the same as any other horse, especially if the PPID is well controlled on treatment.
What is the prognosis for pituitary pars intermedia dysfunction?
The prognosis for horses diagnosed with PPID is variable. Some horses respond to a low level of medication, while others need a much higher level. Earlier diagnosis may result in a better quality of life, particularly if negative consequences like infections and laminitis can be avoided.
How can pituitary pars intermedia dysfunction be prevented?
Prevent PPID by looking for the signs described above. This includes monitoring shedding and comparing to herdmates to detect delayed shedding, especially in older horses. Monitor for decreased energy levels, development of a potbellied appearance or loss of topline, or recurrent foot abscesses or other infections. Regular veterinary examinations 1-2 times a year are also key as they can help evaluate for gradual changes that may be easy to overlook on a day-to-day basis.
For more information:
*This article may not be reproduced without the written consent of the UC Davis Center for Equine Health. Please email requests to [email protected].