

Cervical Vertebral Compressive Myelopathy (CVCM)
What is cervical vertebral compressive myelopathy?
Takeaways
- Cervical vertebral compressive myelopathy (CVCM or CVM) is a developmental defect of the vertebrae in the neck that causes narrowing of the spaces in the spine.
- It is one of the most common noninfectious causes of spinal ataxia in the horse.
- CVCM is also known as “wobbler syndrome” because affected horses are often unsteady on their feet.
- Medical management or surgery may be recommended to treat CVCM, depending on a variety of factors.
- Prognosis varies, with younger horses with mild clinical signs of short duration the most likely to successfully return to performance.
Cervical vertebral compressive myelopathy (CVCM or CVM) is a developmental defect of the vertebrae in the neck (cervical vertebrae) that causes narrowing of the spaces in the spine. It results from lesions that lead to compression of the spinal cord and damage to spinal cord tracts. One of the most common noninfectious causes of spinal ataxia in the horse, CVCM is commonly referred to as “wobbler syndrome” since affected horses are often unsteady on their feet. Other names for this condition include cervical vertebral malformation, cervical vertebral instability, cervical spondylotic myelopathy, and cervical vertebral stenosis.
A number of causes, including malformation of the vertebral column, osteochondrosis, repetitive microtrauma, and dietary factors such as copper deficiency, excessive zinc, or high carbohydrate ration, can result in clinical signs characteristic of CVCM. Male horses appear to be at increased risk for the disease, but the reason for this is unknown. It has been suggested that certain breeds are genetically predisposed to CVCM, but to date no causative mutations have been identified and further evaluation is needed.
What are the clinical signs of cervical vertebral compressive myelopathy?
Clinical signs of CVCM can be mild in the beginning and include stiffness in the neck and mild proprioceptive deficits (inability to correctly place feet). Signs can become more severe as the spinal cord becomes more compressed, developing into ataxia, or incoordination, toe dragging, and decreased range of motion. Proprioceptive defects are typically more severe in the hind (pelvic) limbs than the front limbs.
How is cervical vertebral compressive myelopathy diagnosed?
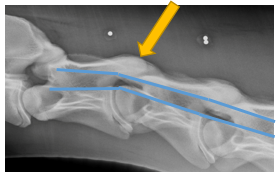
Diagnosis of CVCM typically includes evaluation of a horse’s history, along with physical and neurological examinations. Other causes for ataxia in horses, such as infectious diseases, must be ruled out. Imaging in the form of radiographs (x-rays), computed tomography (CT), or magnetic resonance imaging (MRI) may be employed. A myelogram and laboratory testing of the cerebrospinal fluid (CSF) may be utilized to further evaluate the spinal cord; however CSF cell count and protein are often normal. A CT myelogram is the best available antemortem diagnostic imaging modality to visualize vertebral abnormalities resulting in compression.
If these diagnostic tests are inconclusive, it can be difficult to differentiate CVCM from eNAD/EDM.
How is cervical vertebral compressive myelopathy treated?
Recommended treatment for CVCM depends on the type and severity of the lesion, the duration of clinical signs, and the horse’s age. Medical management can be used in the time immediately following the onset of clinical signs to reduce swelling, thereby reducing compression of the spinal cord.
Management for “controlled growth”, including restricted diet (limited protein and carbohydrates) and exercise (stall rest), may improve CVCM in horses that are younger than 1 year of age. It is important to ensure that the diet still meets minimum nutritional requirements.
Options for medical therapy are more restricted in adult horses with compressive lesions of the spinal cord and are generally restricted to intra-articular injections of corticosteroids and/or hyaluronic acid to reduce swelling, alleviate pain if present, and prevent bony proliferation. However, these treatments rarely improve neurologic status.
Surgical intervention to stabilize the vertebral joints in question can be controversial due to reported high rates of complications in some studies and variable reported postoperative outcomes. Factors such as whether the horse is a good surgical candidate due to its age and the number of compression sites, rehabilitation, the owners’ recovery and performance expectations, costs, insurance, safety and liability issues factor into the decision.
One surgical option for CVCM is cervical stabilization with ventral inter-body fusion, also known as “basket surgery”. The procedure consists of inserting a stainless steel basket (Bagby basket) or kerf cut cylinder (KCC) packed with autogenous bone graft (bone taken from somewhere else in the body) in the area with the lesion. This approach leaves a core of bone to encourage bone growth through the implant, with the remaining spaces filled by the bone graft. Potential complications include vertebral body fracture and implant migration. This surgery is not suitable for every case, and its consideration should be tailored for the specific individual.
Another commonly advocated surgery for CVCM is subtotal dorsal laminectomy, in which a portion of bone is removed from the vertebrae to relieve pressure on the spinal cord. This is a difficult surgical approach that requires substantial expertise to perform. Postoperative complications such as fractures, hematomas and meningitis have been reported.
Additional surgical options include locking compressing plates and screw and rod constructs. These alternative methods may have limited applications, and clinical trials are ongoing.
What is the prognosis for cervical vertebral compressive myelopathy?
The prognosis for CVCM varies based on a number of factors including age of the horse, severity and duration of clinical signs, and the expected level of performance. Reports indicate that horses may improve by one to two grades (out of five), but there is a low probability that they will improve by three or more grades. This means that horses that are severely affected (4 or 5) likely will not regain normal neurologic function.
Younger horses with mild clinical signs of short duration appear to be the most likely to successfully return to performance. Adherence to a structured post-surgery care and rehabilitation plan has been shown to be essential to successful recovery.
How can cervical vertebral compressive myelopathy be prevented?
A genetic component of CVCM is likely, but remains elusive, despite ongoing research efforts. Since this condition is potentially heritable, affected horses should not be bred.
Two causes of CVCM that are possible to control to some extent are nutritional imbalance and physical injury/trauma. Work with a veterinarian and/or equine nutritionist to ensure that horses receive a balanced ration that meets the nutritional needs for their developmental stage. Avoid situations in which young horses, especially, could injure themselves.
For more information
Hales, E.N., Aleman, M., Marquardt, S.A., Katzman, S.A., Woolard, K.D., Miller, A.D., Finno, C. J. 2021. Postmortem diagnoses of spinal ataxia in 316 horses in California. Journal of the American Veterinary Medical Association. 258(12):1386-1393.
*This article may not be reproduced without the written consent of the UC Davis Center for Equine Health. Please email requests to [email protected].